Introduction
•This paper has analyzed the movements involved in rising from a knee-high chair in 12 healthy men weighing within ±10% of standard body weight. A regular series of transition points was observed in the angles of the hip, knee, and ankle joints throughout the sit-to-stand movement, which was classified into six stages.
•The ability to stand from a sitting position., of course, makes other vital activities such as walking possible. Patients who are unable to stand not only are severely limited in terms of daily activities: they present a greater burden to those who must care for them.
Aims of this study
1. How do the angles oft he lower limbs change throughout the process of rising from a chair. and how are these angles affected by the speed of rising (Trial 1).
2. How much hip and knee extension torque is required per kilogram of body weight to complete the sit-to-stand movement (Trial 2).
3. During the sit-to-stand movement, how much load is being eserted on the muscles required for extension (Trial 3).
Trial 1: Measurement of Course-of-Time Changes in the Angles of the Hip, Knee, and Ankle Joints during Sit-to-Stand Movement•Subjects were asked to place their feet flat on the floor at shoulder’s width, and to stand with arms folded.


•The ability to stand from a sitting position., of course, makes other vital activities such as walking possible. Patients who are unable to stand not only are severely limited in terms of daily activities: they present a greater burden to those who must care for them.
Aims of this study
1. How do the angles oft he lower limbs change throughout the process of rising from a chair. and how are these angles affected by the speed of rising (Trial 1).
2. How much hip and knee extension torque is required per kilogram of body weight to complete the sit-to-stand movement (Trial 2).
3. During the sit-to-stand movement, how much load is being eserted on the muscles required for extension (Trial 3).
Trial 1: Measurement of Course-of-Time Changes in the Angles of the Hip, Knee, and Ankle Joints during Sit-to-Stand Movement•Subjects were asked to place their feet flat on the floor at shoulder’s width, and to stand with arms folded.
• The chair was adjusted to knee height for each subject and legs were positioned before standing so that dorsiflexion of the ankle joint was 15’ (fig I ).
• Vectors were analyzed every 0.05 seconds so that changes in leg joint angles could be calculated while the subject was in motion.
• The categories were as follows:
- (1) Fast sit-to-stand (0.8-I .4 seconds) (F-Stand)
- (2) Slow sit-to-stand (3.0-4.0 seconds) (S-Stand)
- (3) Natural sit- to-stand ( 1.7-1.3 seconds) (N-Stand).
• The categories were as follows:
- (1) Fast sit-to-stand (0.8-I .4 seconds) (F-Stand)
- (2) Slow sit-to-stand (3.0-4.0 seconds) (S-Stand)
- (3) Natural sit- to-stand ( 1.7-1.3 seconds) (N-Stand).
Trial 2: Computation Models of the blinimum Unilateral Hip Joint and Knee Joint Extension Torque Required to Complete the Sit-to-Stand Movement
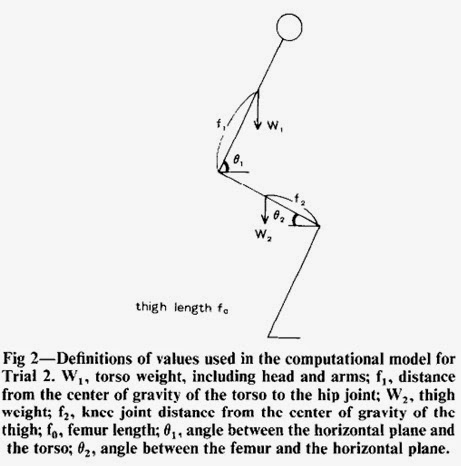
• At a given moment. the value for expressing torque for flexion ofthe hip joint is as follows (when force is applied by the weight of the torso):
H = w1f1*cos(theta1)/2 (fig 2).
• Similarly, the torque for flexion of the knee joint using the weight of the torso and thigh is:
K = w1(f0*cos(theta2) - f1*cos(theta1))/2 + w2f2*cos(theta2).
• If only the following factors involving torque at the hip joint and knee joint are considered, the subject should be able to stand if torque is maintained in the direction of joint extension throughout the standing process
• It must be noted, however. that the success of this theoretical model depends on the assumptions presented in table 1
During N-Stand, the subject must be able to exert extension torque in excess of Hmax and Kmax at each joint throughout the sit-to-stand movement.
In this respect, therefore, Hmax and Kmax represent the minimum unilateral joint extension torque required for completing the sit-to-stand movement.

Results of Trial 1
• Figure 4 shows the average percentage of time spent on each stage by the I2 healthy subjects

Calculate of H
Calculate of K
• Knee extension torque was at its greatest when the buttocks left the chair (T3), then gradually decreased.

Discussion
•Standing is an act of voluntary muscle control, and movements may be altered by the individual at will; in this study, however, a definite pattern was seen when able-bodied people stood up without thinking.
• This system of classification enabled us to determine more accurately the stage at which patients experience difficulty.
• In general, the inability to stand may result from one or more of the following:
- (I) loss of muscle strength
- (2) paralysis or muscle coordination disorders:
- (3) loss of balance;
- (4) neurological or psychological disorders leading to a lack of interest in physical activity; and
- (5) pain in the joints, limited range of motion,6 and other factors.
• Whatever the cause. a loss of muscle strength always follows.
•Standing is an act of voluntary muscle control, and movements may be altered by the individual at will; in this study, however, a definite pattern was seen when able-bodied people stood up without thinking.
• This system of classification enabled us to determine more accurately the stage at which patients experience difficulty.
• In general, the inability to stand may result from one or more of the following:
- (I) loss of muscle strength
- (2) paralysis or muscle coordination disorders:
- (3) loss of balance;
- (4) neurological or psychological disorders leading to a lack of interest in physical activity; and
- (5) pain in the joints, limited range of motion,6 and other factors.
• Whatever the cause. a loss of muscle strength always follows.
• Standard muscle strengthening exercises using weights or muscle exercisers may be inappropriate therapy in the rehabilitation of some patients with symptoms of muscular atrophy. In many such cases it may be better to focus on muscle training that involves repetition of basic movements. Standing, an activity of inestimable value to the patient. should definitely be incorporated in such therapy programs.
• As elderly and disabled populations continue to grow. we recognize the impact that a common activity such as rising from a seated position can have concerning the quality of life. A basic understanding of the sit-to-stand movement is therefore an essential component to rehabilitation studies.